

YOURS QUESTIONS ABOUT HAIR LOSS
Abstract
Hair loss is a normal process (45 to 60 hairs/day), the hair that falls out is continuously replaced by newly grown hair. We lose more hair towards the end of summer and in spring. Hair loss of more than 60 hairs/day is considered abnormal.
Hair loss has very diverse causes.
Diffuse hair loss is mostly encountered in common baldness (male-pattern and female-pattern alopecia) or telogen effluvium (high fever, pregnancy, medication or severe diet). Anagen effluvium causes rapid hair loss after cancer chemotherapy or during alopecia areata. Genetic hair loss can be observed in newborns but mostly appears during childhood (monilethrix, loose anagen hair syndrome, ectodermal dysplasia).
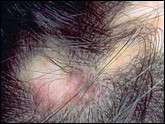
Localized hair loss occurs in male-pattern androgenetic alopecia (in various patterns), fungal infections (tinea), alopecia areata, cicatricial alopecia (lupus erythematosus, lichen plano pilaris, folliculitis decalvans, central centrifugal cicatricial alopecia, postmenopausal frontal fibrosing alopecia, etc.) or can be due to traction alopecia (trichotillomania, braiding and hair straightening). Tumours and skin outgrowths also induce localized baldness (sebaceous nevus, basal cell carcinoma, squamous cell carcinoma).
Stress has often been pointed at as causing hair loss but this has never been confirmed by scientific studies. However, anyone can experience stress and its role should not be neglected when faced with a sizeable hair loss in the weeks following an intense emotional upheaval.
Effective treatment of hair loss is based on finding the cause of the disorder.
• Telogen effluvium can be induced by an iron or vitamin B12 deficiency or a thyroid gland disorder which need to be treated. However, it often resolves spontaneously within 3 or 4 months (after pregnancy, fever, surgery, etc.). In the case of medication-induced telogen effluvium (isotretinoin, cholesterol-lowering drugs, anticoagulants), the causative treatment must be discontinued and replaced with an alternative whenever possible.
• Chemotherapy-induced anagen effluvium can be somewhat minimized by the use of preventive measures (cooling caps).
• Skin diseases and systemic disorders leading to hair loss must be treated in the appropriate manner and according to each case. Tinea infections require oral antifungal therapy. Topical, intralesional or systemic corticosteroids are indicated in the treatment of lichen, synthetic antimalarials (Plaquenil) can also sometimes be useful. Cicatricial alopecia is difficult to treat and requires the intervention a scalp specialist. Once the pathologic process has been stabilized, hair transplantation can sometimes be considered.
• Hair transplantation or a hairpiece can sometimes be helpful in congenital alopecia.
• Alopecia areata in small patches often resolves quickly without treatment (although there may be relapses), whereas more severe alopecia areata must be treated as soon as possible with topical (lotion), intralesional (scalp injections) or more rarely systemic corticosteroids. PUVAtherapy, dithranol (anthralin) and immunotherapy with diphencyprone are often useful.
• Male-pattern androgenetic alopecia improves with finasteride (Propecia®) and minoxidil 5%; dutasteride is still being tested in this indication and only temporary results are available. Hair transplantation remains the sole means of recovering natural hair, the current follicular unit transplant techniques give excellent results when performed by specialist teams. Female-pattern androgenetic alopecia is a common condition, its treatment includes minoxidil 2% and antiandrogens (cyproterone acetate) in case of obvious hyerandrogenism; finasteride is not currently approved in women, it is however being tested in postmenopausal women.
| DIFFUSE HAIR LOSS | Children | Women | Men |
|
Fast or progressive
|
• Congenital alopecia
• Hair dysplasia • Telogen effluvium |
• Androgenetic alopecia • Telogen effluvium |
• Androgenetic alopecia
• Telogen effluvium |
|
Brutal
|
• Chemotherapy
• Alopecia areata |
• Chemotherapy
• Alopecia areata |
• Chemotherapy
• Alopecia areata |
| LOCALIZED HAIR LOSS | Children | Women | Men |
|
From birth
|
• Benign congenital alopecia
• Neonatal occipital alopecia |
• Congenital alopecia
|
• Congenital alopecia
|
|
Progressive
|
• Hair dysplasia
|
• Endocrine disorder
|
• Androgenetic alopecia
|
|
Brutal
|
• Alopecia areata
• Radiotherapy |
• Alopecia areata
• Radiotherapy |
• Alopecia areata
• Radiotherapy |
|
Hair breakage
|
• Tinea infection
• Trichotillomania • Hair dressing and hair care |
• Trichotillomania
• Hair dressing and hair care |
|
|
Scalp involvement
|
• Tinea infection
• Cicatricial alopecia |
• Cicatricial alopecia
|
• Cicatricial alopecia
|
Synonyms
hair loss, effluvium, alopecia, baldness
Related terms
androgenic alopecia, androgenetic alopecia, alopecia areata, cicatricial alopecia
Photographs
|
|||



|
Male-pattern baldness
|
Female-pattern baldness
|
Female-pattern baldness
|
|
|||



|
Alopecia areata-patchy pattern
|
Alopecia areata-ophiasis pattern
|
Alopecia areata totalis pattern |
|
|||



|
Cicatricial alopecia from braids
|
Central centrifugal cicatricial alopecia |
Pseudopelade of Brocq
|
|
|||


|
Lichen planopilaris
|
Frontal fibrosing alopecia
|
Lupus erythematosus
|
Informations
Patient Support Groups
• National Alopecia Areata Foundation – A non profit organization dedicated to providing information about alopecia areata. With support groups in the USA and contacts with similar support groups worldwide.
• Delaware Valley Alopecia Support Group – Support and ideas for those with the condition of alopecia areata, alopecia totalis, and alopecia universalis.
Clinical trial
Consultations
Research
• Etude génétique sur la pelade
Documentation
• Olsen EA. Disorder of hair growth – Diagnosis and treatment. Mc-Graw-Hill; 2003.
• Burden of hair loss – Stress and the underestimated psychosocial impact of telogen effluvium and androgenetic alopecia. Hadshiew IM, Foitzik K, Arck PC, Paus R. J Invest Dermatol. 2004 Sep; 123(3):455-7.
• Can alopecia areata be triggered by emotional stress ? – An uncontrolled evaluation of 178 patients with extensive hair loss. Van der Steen P, Boezeman J, Duller P, Happle R. Acta Derm Venereol. 1992 Aug; 72(4):279-80.
• Postmenopausal frontal fibrosing alopecia – Scarring alopecia in a pattern distribution. Kossard S. Arch Dermatol. 1994; 130:770-774.
• Alopécie frontale fibrosante post-ménopausique – 20 cas. Vaisse V, Matard B, Assouly P, Jouannique C, Reygagne P. Ann Dermatol Venereol. 2003 Jun-Jul; 130(6-7):607-10. French.
• Frontal fibrosing alopecia in postmenopausal women – Tosti A, Piraccini BM, Iorizzo M, Misciali C. J Am Acad Dermatol 2005; 52(1):55-60.
• Treatment of Hair Loss – Price VH, Review Article. N Eng J Med 1999; 341:964-973.
• Update on primary cicatricial alopecias – Ross EK, Tan E, Shapiro J. Journal of the American Academy of Dermatology – July 2005 (Vol. 53, Issue 1, Pages 1-37).
• Evaluation and treatment of male and female pattern hair loss – Olsen EA, Messenger AG, Shapiro J, Bergfeld WF, Hordinsky MK, Roberts JL, Stough D, Washenik K, Whiting DA. Journal of the American Academy of Dermatology. February 2005 (Vol. 52, Issue 2, Pages 301-311).
Websites
• Androgenetic Alopecia – Feinstein R. In: Burg G, Elenitsas R, Quirk C, Elston, Dirk M., editors. Diseases Of The Adnexa: emedicine; oct 2003.
Effluvium télogène
• Telogen effluvium – Hughes E, C, W. Telogen Effluvium. In: Sperling L, Butler DF, Chan E, F., Quirk C, Elston D, M., editors. Diseases Of The Adnexa: emedicine; 2004.
Effluvium anagène
• Anagen effluvium – Seiff B, D., Schwartz R, A., Gascon P. Anagen Effluvium. In: Burg G, Elenitsas R, Quirk C, Elston, Dirk M., editors. Diseases Of The Adnexa: emedicine; aug 2002.
Alopecia areata
• American Academy of Dermatology – Patients pamphlet
• Alopecia Information And Resources – Summaries on different hair loss conditions plus dermatological and alternativetreatments. Includes abstracts of relevant articles from medical journals.
Scientific articles
• Alopecia Areata – Bolduc C, Lui H, R In: Burg G, Elenitsas R, Quirk C, Elston, Dirk M., editors. Diseases Of The Adnexa: emedicine; sept 2002.
e-medicine
• Perifolliculitis Capitis Abscedens et Suffodiens
• Trichorrhexis Invaginata (Netherton Syndrome or Bamboo Hair)
• Dermatlas
Research
• European Hair Research Society – The European Hair Research Society (EHRS) web site. A non-profit organization dedicated to the advancement of hair research. Extensive links lists for dermatology clinics and articles about hair and hair loss.
• North American Hair Research Society
• Australian Hair and Wool Research Society (http://www.ahwrs.org.au) – A not-for-profit organisation founded in 1996. Australia and New Zealand both have a long and proud history of achievement in scientific wool research.
Definitions
Anagen:
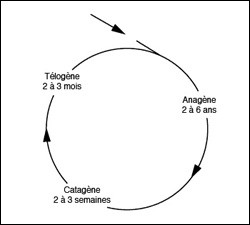
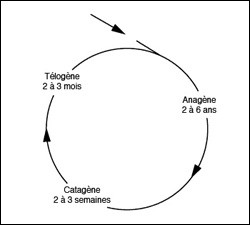
The anagen or growth phase of the hair cycle involves 80 to 90% of the hair and lasts from 2 to 6 years (3 years/1000 days in men and 5 years in women). The duration of this phase determines the final length of the hair, which grows at a speed of 0.4 mm/day (i.e. 1 cm/month).
Anagen effluvium:>Abnormal hair loss during the anagen or growth phase. Anagen effluvium is the least common type of hair loss and mostly occurs following a course of medication interfering with the hair formation process (e.g. chemotherapy), or in alopecia areata.
Androgenetic alopecia (AGA):>Male or female-pattern androgenetic alopecia is also known as common baldness or androgenogenetic alopecia. This type of hair loss is due to aging and is characterized in males by progressive balding of the crown of the head and the forehead, whereas in women hair loss mostly affects the crown. Nevertheless, diffuse hair loss can also occur in male-pattern androgenetic alopecia whereas female-pattern alopecia can sometimes induce hair loss on the sides of the forehead.
Catagen:>The catagen phase is the intermediate or “resting” phase of the hair cycle, lasting for 3 weeks and involving 0 to 2% of the hair mass. This phase is intermediate between the anagen or growth phase and the telogen “shedding” phase of the hair cycle.
Cicatricial alopecia:>Permanent hair loss; can be due to congenital malformation (congenital aplasia, angioma), trauma (wound, burn or surgery), scalp disease (lupus erythematosus, lichen planus) or scalp tumour (basal cell carcinoma, squamous cell carcinoma) leading to the formation of abnormal scar-like tissue.
Congenital:>Present at birth.
Diffuse alopecia:>Overall decrease in hair density.
Exogen:>The exogen phase is a subphase of the telogen phase, during which the hair falls out. Roughly 1% of the hair in the telogen phase falls out every day.
Hair dysplasia:>Abnormality of hair structure.
Hair cycle:>The different stages of evolution of human hair. The anagen or growth phase involves 80 to 90% of the hair and lasts for 2 to 6 years. During the catagen phase the hair stops growing; this phase lasts for 2 to 3 weeks and involves 0 to 2% of the hair mass. Lastly, the telogen or shedding phase involves 10 to 20% of the hair and lasts for about 2 to 3 months, after which the cycle starts again. All abnormal hair loss is characterized by an alteration in the hair cycle pattern.
|
|
|
|
Hair follicle:
All the elements forming a hair. Hair follicles are made up of a hair shaft (the hair itself) and a sebaceous gland and arrector pili muscle attached to it. Hair follicles are grouped together in follicular units containing 1 to 4 hair shafts.
Localized alopecia: Localized decrease in hair density.
Normal hair loss: Hair shedding is a continuous and normal process. Normal hair loss is characterized by the shedding of 45 to 60 hairs a day, it reaches its climax at the end of summer and in spring.
Scalp:> Skin covering the skull and containing hair follicles.
Telogen: The telogen phase of the hair cycle is characterized by the involution and shedding of the hair, it involves 10 to 20% of the hair and lasts for around 3 months (100 days). Roughly 1% of the hair in the telogen phase of the cycle fall out each day (exogen phase).
Telogen effluvium:> The growing or involuting hair is rushed into shedding (exogen phase) or the growing hair is rushed into involution followed by shedding. Telogen effluvium can occur a few weeks after childbirth, surgery, high fever or certain medical treatments, it is also encountered during attacks of androgenetic alopecia.
Tinea: Tinea or ringworm is an infection of the hair or facial hair (sycosis) due to dermatophytic fungi.
Traction test:> Test during which the health practitioner pulls out gently but firmly on a strand of 25 to 30 hairs. The shedding of more than 5 hairs is considered abnormal.
Trichogram: Diagnostic test aiming at quantifying hair loss, establishing which type of hair loss is present (telogen or anagen effluvium) in order to refer the patient or to diagnose their condition. A strand of hair is taken from the forehead, temples and neck using tweezers. The hair is examined microscopically and classified according to its type (anagen, catagen, telogen). The rate of shrinking of the hair can also be assessed, as well as the occurrence of dystrophic bulbs, which are found in alopecia areata or anagen effluvium.
Trichotillomania: Irrepressible need of pulling or twisting one’s hair leading to hair breakage and hair loss. This tic is considered as being part of obsessive compulsive disorder (OCD).
|
|
|
|
Congénital : présent à la naissance.
Dysplasie pilaire : anomalie de la structure du cheveu.
Effluvium anagène : indique une chute de cheveux importante. Le cheveu chute au cours de sa phase de croissance. Cette variété de chute de cheveux est la plus rare et survient le plus souvent après la prise de médicaments comme les chimiothérapies qui interfèrent avec la fabrication du cheveu ou bien au cours de la pelade.
Effluvium télogène : indique une chute de cheveux importante et passagère. Les cheveux en phase de croissance ou d’involution sont précipités en phase de chute (phase exogène) ou bien les cheveux en phase de croissance sont précipités en phase d’involution puis de chute. L’effluvium télogène se rencontre quelques semaines après un accouchement, une opération, une fièvre élevée ou la prise de certains médicaments, mais peut aussi se voir au cours d’une poussée d’alopécie androgénique.
Exogène : la phase exogène est un moment particulier de la phase télogène où les cheveux chutent. Environ 1% des cheveux en phase télogène sont perdus chaque jour.
Follicules pileux : il s’agit de l’ensemble des éléments qui constituent un cheveu ou un poil. Le follicule pileux comporte une tige pilaire (le cheveu ou le poil proprement dit), la glande sébacée et le muscle arrecteur du poil qui lui sont annexés. Les follicules pileux sont groupés en unités folliculaires qui comportent de 1 à 4 tiges pilaires.
Greffe de cheveux : la greffe de cheveux est une technique chirurgicale qui permet d’implanter sur la zone dégarnie d’un sujet, des cheveux prélevés à l’arrière du cuir chevelu sur lui même.
Télogène : la phase télogène est la phase où les cheveux involuent et chutent, elle touche 10 à 20 % de la chevelure et dure environ trois mois (100 jours). Ainsi, 1% des cheveux en phase télogène sont perdus chaque jour au cours de la phase exogène.
Teigne : la teigne désigne une infection des cheveux ou des poils de la barbe (sycosis) provoquée par des champignons du genre dermatophytes.
Test de traction : test où le médecin tire sur une mèche de 25 à 30 cheveux fermement, mais sans brutalité. Au cours de ce test, une chute supérieure à 5 cheveux est considérée comme excessive.
trichochogramme : examen complémentaire qui permet de quantifier une chute de cheveux, de la classer parmi les diverses formes (effluvium anagène, télogène) et d’orienter ou de faire un diagnostic. Une mèche de cheveux est prélevée dans les régions du front, des tempes et du cou avec une pince. Les cheveux sont ensuite examinés au microscope et classés selon leur type (anagène, catagène, télogène, on peut aussi apprécier leur taux de miniaturisation et l’existence de bulbes dystrophiques qui se rencontrent au cours de la pelade et des effluvium anagènes.
Trichotillomanie : envie irrésistible de tirer ou tordre ses cheveux qui aboutit à une chute de cheveux avec des cheveux cassés. Cette habitude est classée dans le cadre des troubles obsessionnels compulsifs (T.O.C) ou des troubles du contrôle des impulsions.